Contributing factors
The development of a prolapse has been determined multi-factorial.A number of factors that contribute to the development of a prolapse are well established, others are potential risk factors. Given the conditions in which Nepali women are living, especially in rural areas, most contributing factors are more pronounced and of specific importance.
Factors directly associated with a higher risk of developing POP are: a first pregnancy at young age, a higher number of deliveries, delivery without professional assistance, insufficient rest after delivery, malnutrition, heavy workload and increased abdominal pressure due to a cough, constipation, obesity or hard physical exertion.26,9
All these factors do not differ from factors related to POP in western countries but are more explicitly present in women living in rural Nepal. For example, the percentage of undernourished women is 13.2% in Hill and Mountain area and 31.7% in Terai area. Resuming “heavy physical work”, such as farm work, within two to three weeks of giving birth occurred with about 80% of women in the Hills and Mountains. In the Terai about 34% of women resumed “heavy physical work” within one week and another 40% within two to three weeks.3 On the other handan intriguing finding is that levator and sphincter trauma are significant less prevalent in Nepali women in comparison to Western population.18
These and many more substantial variations of these figures point to the important insight that these factors reflect other issues such as the lack of education and information and lack of ante- and postnatal care.2These in turn are linked to fundamental issues such as poverty and a patriarchal societal construct. These issues are interdependent, being both causes and effects with a complex chain of feedback loops. In addition genetic makeup may be a direct predisposing factor and its effects can be magnified by the other causes. See fig 4.
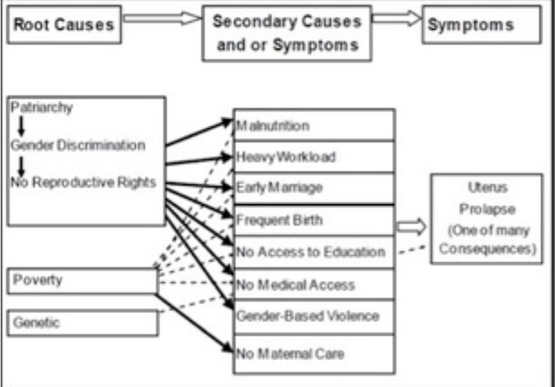
fig 4
Root and Symptomatic Causes of POP from WRRP Unheeded Agonies 2007
This is also illustrated by lack of knowledge about disease, treatment possibilities and lack of treatment, are main causes of POP in women in rural Nepal.9,16
Most participants (women, health workers) in a survey did not recognize POP symptoms.10Women are also frequently not aware of which factors increase their risk of POP. And even when they are aware, they are often unable to exercise control over their lives and reduce their exposure to the risk factor. Social structure, caste, ethnic, religious, and regional identities have a significant effect on how women and girls experience the possibility to act upon the mentioned risk factors.21




© Vrouwen voor Vrouwen | website: hostnet | foto's Nepal: Lizet Sleutelberg


